Winick, Reid L. Cranial electrotherapy stimulation (CES): a safe and effective low cost means of anxiety control in a dental practice. General Dentistry. 1999; 47(1):50-55.
Device
Alpha-Stim
Key Variable
Anxiety
Objective
To evaluate the effect of CES on dental patients’ anxiety when compared to sham treatment under the same experimental conditions in subjects meeting the inclusion and exclusion criteria.
Design
This was an IRB approved, randomized, sham controlled, double-blind, clinical trial. The subjects, investigator and staff were all masked as to the identity of the device.
Primary Effectiveness Endpoint
The primary effectiveness endpoint was the change from baseline measures of anxiety scores compared to the sham group at the completion of the dental procedures.
Key Inclusion Criteria
1. Dental patients having common dental surgical procedures.
2. Male and female subjects ≥ 20 years of age.
3. Must report having anxiety about the dental procedure.
Key Exclusion Criteria
• Pregnancy
• Presence of implanted pacemakers, pumps or stimulators
• Persons who reported no anxiety about the dental procedure were excluded from this study.
Protocol Summary
Patients were randomly assigned to the active CES group (N = 16), or sham CES (N = 17) group in the order they arrived for various dental procedures. A “double-blinding box” provided by the manufacturer of the Alpha-Stim CES device was used so neither the patient nor the dentist was aware of who was receiving actual stimulation. The 100 mm Visual Analogue Scale (VAS) of “not anxious” on the left to “very anxious” on the right was used at baseline, midpoint of the procedure and at the endpoint of the dental procedures by both the patient and dentist, and an inverse 7 point Likert scale with 1 “more anxious” to 7 “less anxious” was used at the conclusion of each treatment as a method to corroborate the findings from the VAS scale. On the VAS a higher score indicated more anxiety while on the inverse Likert scale a lower scale indicated more anxiety.
Device Application Protocol
Subjects were randomized to either the active or sham groups in the order that they arrived at the dental office. Baselines measures were done just prior to the active or sham CES treatment. Outcome measures were done at mid-point in the procedure and endpoint measures were done right after the completion of the procedure. The active CES device was pre-set at 200 µA and the sham CES device was set to “0” so the ear-clip electrodes did not emit electricity. The time on both the active and sham devices was set to “continuous,” so the CES treatment continued until the procedure was done.
Study Blinding
The subjects, investigator and staff were all masked as to the identity of the device.
Results
Subjects
A total of 33 subjects, 9 males and 24 females, 20 to 59 years old, completed the study.
Baseline Measurements
Baseline measurements were taken prior to the start of the procedure and before the active CES or sham treatment. There was no significant difference in anxiety levels at baseline between the active and sham groups.
Data Analysis
Data were analyzed using the student t-test (unpaired) comparing the active and sham groups at baseline, mid-point and endpoint of study.
Anxiety
The mean value for the dentist’s and patient’s baseline evaluations tended to be higher in the treatment group at the start probably due to the more severe procedures in that group compared to the sham group, but was not significant. The active CES group had lower anxiety scores (VAS) from baseline to endpoint of the study than the sham group as measured by the investigator (p<.02) and subjects (p<.02), see Figure 1. Findings using an inverse Likert scale corroborated these findings for both the investigator evaluation (p < .01) and subjects’ evaluation (p <.01).
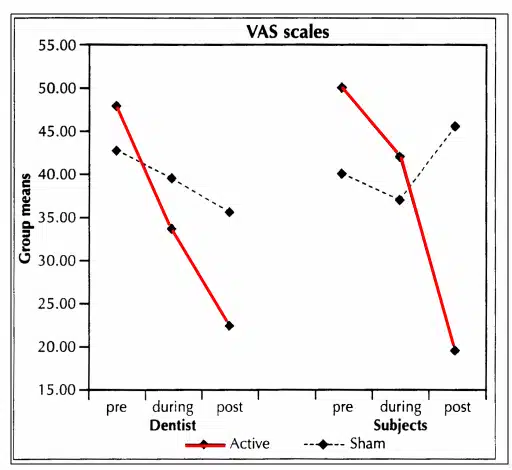
Figure 1. Comparison of group means on VAS anxiety scale by group over time.
Quality of the Research
Strengths of this study include: (1) use of a randomized, sham controlled, double-blind design; (2) active and sham Alpha-Stim devices were pre-set at the designated levels for each specific group for current and time; (3) sham devices were the same as active devices except they did not emit electricity; (4) all subjects had common dental procedures such as fillings, crowns or bridge, or dental exams and cleaning; (5) all subjects reported dental anxiety at baseline in order to be in the study; (6) an inverse Likert scale was used post-test as a method to corroborate the findings from the VAS scale; and (7) the subjects, investigator and staff were all masked as to the condition of the device. The small N (33) in this study could be considered a limitation of the study. However, based on the moderate to large effects sizes for anxiety in the literature, the N of 33 for this study was large enough to detect a significant difference between the active CES and sham CES groups in favor of the active CES group. This study was done in 1999 and the investigator used student t-tests to analysis the data which was common in that time period. Today, an investigator would most likely use repeated measures ANCOVA for data analysis. However, this study showed that CES decreases anxiety and this is consistent with the findings of other Alpha-Stim research that found CES decreases anxiety.
